Systemic manifestations of systemic metabolic disorder
Systemic metabolic disorder encompasses several critical components that are commonly present but varying in intensity, especially in the early stages, before progressing towards a multi-organ systemic metabolic failure that compromises global energy homeostasis. Below, we present the main systemic manifestations of SMD that are included in our proposed staging system.
Insulin resistance, pre-diabetes, and Type 2 diabetes
Insulin resistance happens when the body’s cells no longer respond properly to insulin, causing the pancreas to produce more insulin to keep blood sugar normal. Over time, this can lead to pre-diabetes and eventually Type 2 diabetes when insulin production can’t keep up. Even before diabetes develops, insulin resistance increases the risk of heart disease, fatty liver, kidney problems, and high blood pressure. These effects are driven by inflammation, oxidative stress, and hormonal imbalances that damage organs and blood vessels.
Metabolic dysfunction–associated steatotic liver disease
Metabolic dysfunction–associated steatotic liver disease (MASLD) is a liver condition where excess fat (>5%) accumulates in the liver, often linked to metabolic problems. It can progress from simple fat buildup to inflammation (MASH), fibrosis, cirrhosis, and sometimes liver cancer. MASLD is strongly associated with Type 2 diabetes and may contribute to heart and kidney problems through effects on lipid metabolism. Both the amount and type of liver fat—including saturated fats and certain lipids like ceramides—affect disease progression. Some MASLD forms increase cardiovascular risk, while others are more liver-specific and less harmful to the heart.
Hypertension
Hypertension in systemic metabolic disorders (SMD) is mainly driven by obesity, insulin resistance, and salt intake. Visceral fat releases inflammatory signals that worsen insulin resistance, while insulin and obesity-related changes increase sodium retention and activate the kidneys, sympathetic nervous system, and RAAS, raising blood pressure. Fat around the kidneys and vascular changes further contribute, and liver fat (MASLD) may also play a role through inflammation and insulin resistance.
Atherogenic dyslipidaemia
Atherogenic dyslipidaemia is common in systemic metabolic disorders and is marked by high triglyceride-rich lipoproteins (VLDL and chylomicrons), small dense LDL, and low HDL. It develops due to insulin resistance, increased fat release from adipose tissue, excess liver production of VLDL, impaired lipolysis, and altered cholesterol transfer. This dyslipidaemia increases atherosclerosis risk. Proteins like ANGPTL3 and apoCIII play key roles by inhibiting lipoprotein breakdown, and genetic or pharmacologic alterations in these proteins affect lipid levels and ASCVD risk.
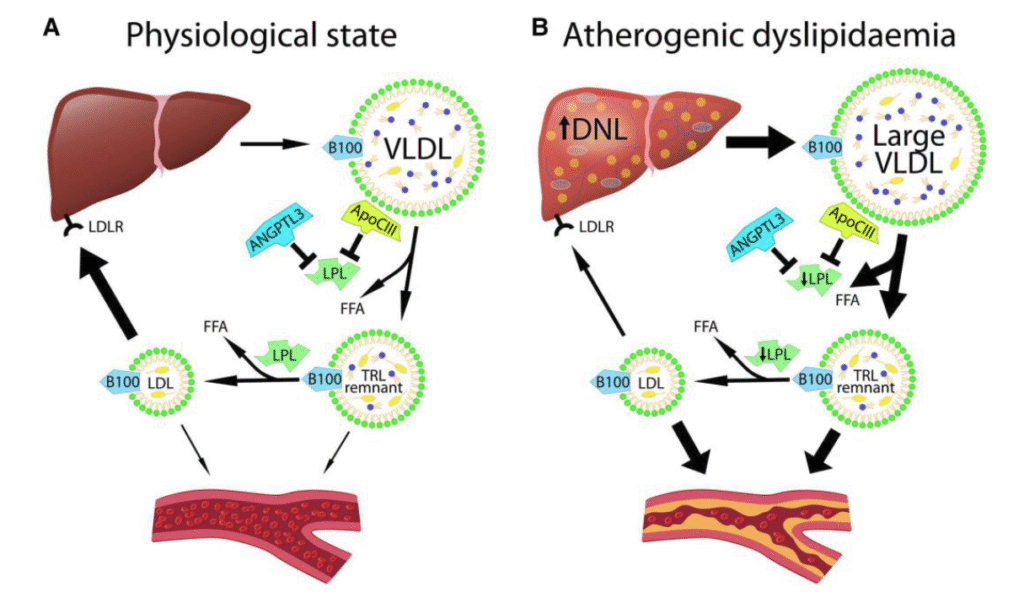
Figure 1
Overview of the development of atherogenic dyslipidaemia. (A) In the physiological state, the liver produces triglyceride-rich apolipoprotein B100-containing very low-density lipoprotein (VLDL). Triglycerides in these particles are hydrolyzed by lipoprotein lipase (LPL) to release free fatty acids (FFA). Both angiopoietin-related protein 3 (ANGPTL3) and apolipoprotein C-III (apoCIII) are endogenous inhibitors of LPL. Delipidation of VLDL results in the formation of triglyceride-rich lipoprotein (TRL) remnants, which are further delipidated to become LDLs. LDL is taken up by the liver through the LDL receptor (LDLR) and thereby removed from the circulation. (B) Atherogenic dyslipidaemia is characterized by increased hepatic de novo lipogenesis (DNL) and secretion of larger, more triglyceride-rich VLDL from the liver, impaired LPL–mediated lipolysis, and reduced uptake of LDL. All these factors lead to increased accumulation of TRL remnants and LDL. Both LDL and TRL remnants can transverse the endothelium and contribute to lesion initiation and progression in artery walls
Inflammation
Visceral fat and insulin resistance often trigger low-grade systemic inflammation, raising the risk of cardiovascular disease. Inflammation arises from stress in fat and liver cells, tissue hypoxia, and gut-derived signals, activating immune pathways (e.g., NLRP3) that release cytokines like IL-1, IL-6, and TNF-α. This chronic inflammation contributes to insulin resistance, liver damage (MASLD), and atherosclerosis. Clinical and genetic studies confirm inflammation’s causal role, making it a key target for improving cardiometabolic health. However, it is important to target the immune systems in a way that prevents an increase in infections.
Heart failure
Obesity and related conditions—insulin resistance, diabetes, hypertension, dyslipidaemia, and inflammation—increase the risk of heart failure. They can lead to HFrEF (reduced ejection fraction) after heart attacks or HFpEF (preserved ejection fraction), which is strongly linked to obesity even without prior heart disease. HFpEF develops through changes in heart structure and function, inflammation, neurohormonal activation, and obesity-related comorbidities. Over 80% of HFpEF patients are overweight or obese, and it is projected to become the dominant form of heart failure.
HFpEF differs between sexes: women are more symptomatic and show different heart remodeling patterns, while men have higher risks of hospitalization and mortality. Sex-specific differences mean standard “normal” measures may underestimate dysfunction in women.
Mechanisms and conditions through which obesity contributes to heart failure with preserved ejection fraction
- Myocardial stiffness and increased chamber stiffness due to structural myocardial change, which may or may not be associated with hypertension
- A pro-inflammatory state associated with visceral adiposity with resultant coronary microvascular endothelial dysfunction and increased oxidative stress, which can lead to cardiomyocyte hypertrophy and fibrosis and to interstitial fibrosis
- Increased blood volume resulting in greater cardiac filling pressures
- Increased cardiac output, stroke volume, stroke work, and hypertension, which can lead to left ventricular hypertrophy or remodelling, including both concentric and eccentric left ventricular hypertrophy/remodelling
- Right ventricular dilatation and dysfunction
- Increased epicardial fat causing right ventricular dysfunction
- Increased pericardial restraint and ventricular interdependence (mechanical factors)
- Left atrial remodelling (left atrial myopathy) and atrial fibrillation
- Increased myocardial work and decreased efficiency with increasing BMI and insulin resistance, possibly related to greater myocardial reliance on fat metabolism versus glucose oxidation
- Decreased exercise capacity (reduced peak oxygen consumption) related to decreased myocardial and skeletal muscle metabolic efficiency and increased filling pressures with exercise
- Impaired venous capacitance with resultant increased stressedblood volume resulting in increased filling pressures
- Sympathetic activation with blood volume redistribution from the splanchnic to the intravascular space
- Autonomic dysfunction leading to chronotropic incompetence
- Activation of RAAS and direct action on the adrenal gland resulting in increased release of aldosterone
- Diabetic cardiomyopathy
- Sleep apnoea, which increases risk of hypertension and atrial fibrillation
- Epicardial coronary artery disease with minor or no ischaemic myocardial damag
Kidney disease
Obesity and related metabolic problems can damage the kidneys, causing chronic kidney disease (CKD), often shown by high urine albumin or low kidney filtration (eGFR). Damage occurs directly through pressure on kidney structures and indirectly via diabetes, hypertension, inflammation, and altered adipokines. CKD is closely linked with heart disease, forming a cardiovascular–kidney–metabolic syndrome, where kidney dysfunction both contributes to and is worsened by cardiovascular problems. Risk is categorized from moderate to very high using established Kidney Disease Improving Global Outcomes (KDIGO) heat map.