European Atherosclerosis Society consensus statement:
Clinical management of HeFH
- Rationale for lowering LDL-C treatment goals in children with HeFH
- Why is it important to focus on cumulative LDL-C exposure?
- Other major risk enhancers that may trigger lower LDL-C treatment goals
- Can cardiovascular imaging support risk stratification in children with HeFH?
- Lifestyle measures
- Pharmacological treatment
- Does sex matter?
- Safety
Rationale for lowering LDL-C treatment goals in children with HeFH
It is increasingly recognized that treatment of FH should focus on reducing the cumulative burden of low-density lipoprotein cholesterol (LDL-C), a key predictor of atherosclerotic cardiovascular disease (ASCVD). Compared with 2015 EAS consensus, we propose starting treatment earlier (in the first decade of life, ideally from 6 years) and treating more intensively to prevent the development of atherosclerosis in childhood.
We also propose an LDL-C treatment goal of ≤3.5 mmol/L (135 mg/dL) in children aged 6 to <10 years, and a lower treatment goal of ≤3.0 mmol/L (115 mg/dL) in children from 10 years or from 6 years if other major risk enhancers are present.
Early use of lipid-lowering therapies (LLTs) is safe, effective, and can reduce arterial changes, supporting prevention of atherosclerosis from childhood. Shared decision making is required to ensure that the optimal treatment strategy is chosen for the individual child, with an emphasis on starting treatment of any intensity before puberty and ensuring adherence to treatment.
A comparison of these modified LDL-C treatment goals with those presented in the 2015 EAS consensus statement is presented in Table 1.
Table 1 Comparison of the LDL-cholesterol (LDL-C) treatment goals proposed in the current consensus and in the 2015 EAS consensus statement for children with FH
| 2015 LDL-C treatment goals | 2026 LDL-C treatment goals |
| Start pharmacological treatment at 8 years | Start pharmacological treatment ideally at 6 years |
| Reduce LDL-C concentration | Reduce LDL-C concentration |
| ◦ by 50% from baseline at 8–10 years | ◦ to ≤3.5 mmol/L (135 mg/dL) at 6–<10 years |
| ◦ to 3.5 mmol/L (135 mg/dL) at >10–<18 years | ◦ to ≤3.0 mmol/L (115 mg/dL) at 10–<18 years or with other major risk enhancers* at 6–<10 years |
Why is it important to focus on cumulative LDL-C exposure?
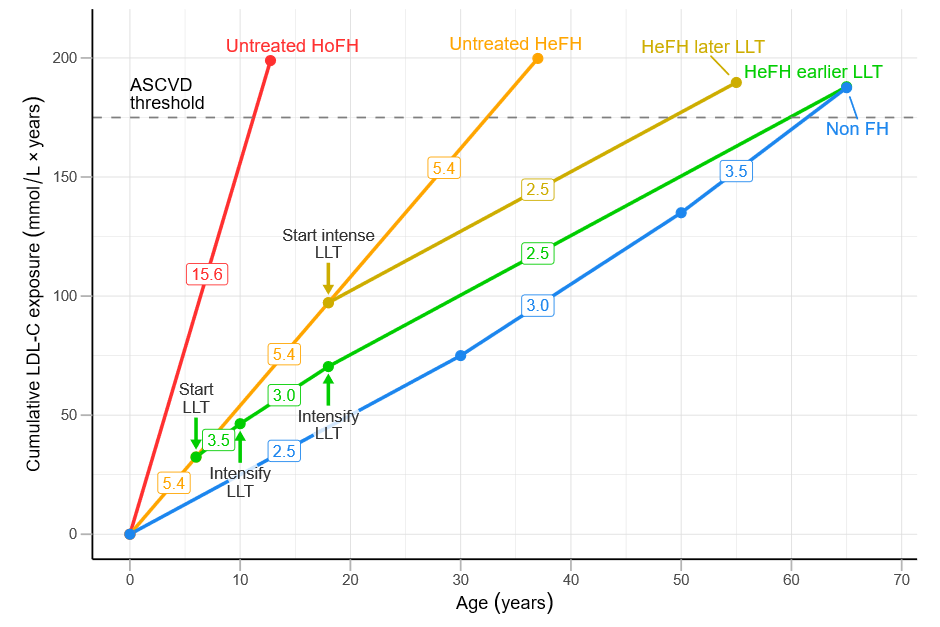
Current treatment guidelines are based on LDL-C concentrations at diagnosis, but the real risk comes from lifelong LDL-C exposure. The risk of symptomatic ASCVD doubles when the cumulative LDL-C crosses a threshold of 175 mmol/L (6800 mg/dL) × years. In people without FH, this threshold is reached on average after the age of 60 years. It is reached much earlier in those with untreated FH: by the age of 33 in those with HeFH and as early as 12 in children with HoFH.
Early, intensive, and consistent treatment with statins (or other lipid-lowering therapies) can significantly delay reaching this risk threshold. It is therefore important to start treatment early, increase the intensity of treatment when appropriate, and continue on treatment to minimise long-term cardiovascular risk.
Other major risk enhancers that may trigger lower LDL-C treatment goals
Other major risk enhancers may warrant lower LDL-C treatment goals in children with FH. The 2015 EAS consensus emphasised treatment and control of additional risk factors, but it did not propose altering LDL-C targets. In the current consensus, lowering the LDL-C treatment goal by 0.5 mmol/L is proposed in children aged 6 to under 10 years with major risk enhancers. Only risk factors that would dramatically increase risk and cannot be corrected by lifestyle have been selected as major risk enhancers.
| Major risk enhancers that prompt lowering LDL-C treatment goals from 6 years |
| ◦ Lipoprotein(a) ≥250 nmol/L (120 mg/dL) – a high concentration associated with a doubled risk of ASCVD in the adult population |
| ◦ Diabetes |
| ◦ Hypertension |
| ◦ Chronic inflammatory diseases |
| ◦ Chronic kidney disease |
| ◦ Kawasaki disease |
| ◦ Human immunodeficiency virus |
| ◦ Cancer survivor |
Lp(a) levels are largely genetically determined and may increase ASCVD risk from childhood. As no paediatric Lp(a)-lowering therapies are currently available, we propose using a high threshold, ≥250 nmol/L (120 mg/dL), to trigger a lower LDL-C treatment goal in children aged 6–<10 years.
Smoking, vaping, and obesity also increase ASCVD risk. Children with HeFH should be discouraged from starting to smoke or vape by discussing the risk at their first visit to an FH clinic. If a child with HeFH already smokes or vapes or has developed obesity, extra lifestyle advice is required rather than striving for lower LDL-C treatment goals.
Can cardiovascular imaging support risk stratification in children with HeFH?
In adults with FH, cardiovascular imaging techniques can provide additional information about future cardiovascular risk. However, these techniques are not recommended for risk stratification in children HeFH.
Lifestyle measures
Lifestyle measures should be the first step in managing children with HeFH, although alone they are usually insufficient to achieve LDL-C treatment goals. Some children are too young when diagnosed to start pharmacological treatment but not too young to be introduced to a healthy lifestyle. Lifestyle measures, implemented in parallel with or followed by timely pharmacological treatment, give the child and their parents a feeling of being in control. In the current era with genetic confirmation of a diagnosis, it is possible to identify children with mild FH-causing variants and LDL-C concentrations close to the treatment goal, who might benefit from lifestyle measures alone.
Regular physical activity should be encouraged, while smoking and vaping should be avoided. Obesity should be avoided and other cardiovascular risk factors should be treated. Nutritional management goals for children with FH are to reduce LDL-C and overall cardiovascular risk while ensuring normal growth and neurocognitive development. Family-based dietary advice and promotion of a healthy diet are proposed rather than focusing solely on food categories.
A cautious low-fat diet has been shown to be safe from in children from 6 months of age. Potential risks to be aware of and avoid include insufficient intake of energy, essential fatty acids and vitamin E, and the development of eating disorders.
Table 2 Dietary components that should be limited or promoted in children with familial hypercholesterolaemia
| Avoid or limit | |
| Dietary cholesterol | 200-300 mg/day |
| Saturated and trans fatty acids: processed foods, animal fat, red meat, whole-fat dairy products, pastries, palm oil, and coconut oil. | <7% Daily Energy Intake (DEI) |
| Added simple sugars, including fructose | <10% DEI |
| Promote | Goals |
| Balanced diet | Carbohydrate 45-60%, fat 25-35%, protein 12-15% of DEI adapted to age |
| Structured complete and regular meals; stress importance of breakfast | |
| Low-fat dairy foods | |
| Long-chain polyunsaturated fatty acids (PUFA): oily fish twice a week, pulses, nuts, seeds, tofu, vegetable oils (rapeseed, soybean, corn, sunflower) | Promote n-3 PUFA; total PUFA 5-10% DEI |
| Monounsaturated fatty acids (MUFA): vegetable oils (rapeseed, olive, canola, peanut, sesame), avocados, nuts and seeds | 10-15% DEI |
| Fibre: fresh fruits and vegetables, wholemeal bread, cereals, legumes | 25-40 g/day, 7-13% soluble fibres |
| Intake of lean and fatty fish, shellfish, lean chicken and turkey (white meat, skinless), limited lean red meat (>93% lean, fat trimmed, free range) |
Pharmacological treatment
Treatment should not only focus on “the lower the better” but also “the earlier and the longer the better”.
Early statin treatment in children with familial hypercholesterolaemia (FH) can reduce atherosclerotic cardiovascular disease (ASCVD) risk to that of the general population. Treatment should focus on both early initiation and long-term LDL-C reduction.
- Table 3 lists the LLTs currently approved in children, the age from which they are approved and the extent of LDL-C reduction to be expected with each therapy.
- A treatment algorithm for children with HeFH is presented in Figure 3.
Table 3 Approved lipid-lowering therapies for children with familial hypercholesterolaemia
| Lipid-lowering therapy | Age approved/tested | Approved (or tested) dose range and route of administration | LDL-C reduction* | Key publications |
| Statins (HMG-CoA reductase inhibitors) | ||||
| Pitavastatin | ≥6 years | 1-4 mg (PO) | 23-39% (placebo adjusted) | Braamskamp et al., 2015 |
| Rosuvastatin | ≥6 years | 5-20 mg (PO) | 35-45% | Braamskamp et al., 2015 Stein et al., 2017 (HoFH) |
| Pravastatin | ≥8 years | 20-40 mg (PO) | 24% (placebo adjusted) | Wiegman et al., 2004 |
| Atorvastatin | ≥10 years | 10-20 mg (PO) | 40% (placebo adjusted) | McCrindle et al., 2003 Raal et al., 2000 (HoFH) |
| Fluvastatin | ≥10 years | 20-80 mg (PO) | 34% | van der Graaf et al., 2006 |
| Lovastatin | ≥10 years | 10-40 mg (PO) | 17-27% (placebo adjusted) | Stein et al., 1999 (in boys) Clauss et al., 2005 (in girls) |
| Simvastatin | ≥10 years | 10-40 mg (PO) | 31-40% (placebo adjusted) | de Jongh et al., 2002 |
| Inhibitor of intestinal cholesterol absorption | ||||
| Ezetimibe | ≥6 years EMA ≥10 years FDA | 10 mg (PO) | 27% as monotherapy (placebo adjusted) 15% on top of simvastatin (placebo adjusted) | Kusters et al., 2015 Van der Graaf et al., 2008 |
| PCSK9 inhibitors | ||||
| Alirocumab | ≥8 years (not approved for HoFH <18 years) | If <50 kg: 150 mg (SC) q4w and 40 mg (SC) q2W If ≥50 kg: 300 mg (SC) q4w and 75 mg (SC) q2W | 34-43% on top of background LLT (placebo adjusted) | Santos et al., 2024 |
| Evolocumab | ≥10 years | 420 mg (SC) q4w and 140 mg (SC) q2w | 38% on top of background LLT (placebo adjusted) | Santos et al., 2020 Santos et al., 2022 Raal et al., 2024 (HoFH) |
| Inclisiran | ≥12 years** | 300 mg (SC) at 0 and 90 days and then q6m | 29-34% on top of background LLT (placebo adjusted) | Wiegman et al., 2026 Wiegman et al., 2025 (HoFH) |
| Bile acid sequestrant | ||||
| Colesevelam | 10 years (avoid in HeFH***) | 1.875-3.75 g (PO) | 6-12% (placebo adjusted) | Stein et al., 2010 |
| ANGPTL3 inhibitor | ||||
| Evinacumab | ≥6 months EMA ≥1 year FDA (approved for HoFH) | 15 mg/kg (IV) q4w | 48% | Wiegman et al., 2024 (HoFH) |
| Microsomal triglyceride transfer protein inhibitor | ||||
| Lomitapide | ≥2 years** (approved for HoFH) | 2-60 mg based on age, weight and tolerability (PO) | 53% | Masana et al., 2024 (HoFH) |
**Approved by the US Food and Drug Administration (FDA) but not yet by the European Medicines Agency (EMA).
***For HeFH, use only in situations when the newer LLTs are not available or tolerated.
PO, oral. SC, subcutaneous. IV, intravenous. LLT, lipid-lowering therapy.
To date, no data are available on the use of the adenosine triphosphate-citrate lyase inhibitor bempedoic acid in children or adolescents; however, a phase 2 trial has recently been completed in children with HeFH aged 6-17 years (NCT05694260).
Statins remain first-line therapy and are generally well tolerated. High-potency statins such as rosuvastatin and atorvastatin are preferred. The dose and/or intensity of statin should be increased according to the LDL-C concentration, residual LDL receptor (LDLR) activity and age-dependent treatment goal. Lipid profile, creatine kinase and aminotransferases (alanine transaminase and aspartate transaminase) should be measured 8–12 weeks after increasing the dose or introducing a (new) statin, and annually thereafter.
| If targets are not achieved with statins: → Add ezetimibe if close to goal (i.e., <4.0 mmol/dL (155 mg/dL)) → Consider a PCSK9 inhibitor instead of ezetimibe if LDL-C remains high (i.e., ≥4.0 mmol/L (155 mg/dL)) |
With current LLTs, treatment goals are usually achievable with ≤2 drugs, while avoiding more complex regimens to support adherence.
- Monoclonal antibody PCSK9 inhibitors (evolocumab, alirocumab) are approved for children with HeFH from 10 and 8 years, respectively; evolocumab is also approved for HoFH from 10 years.
- Inclisiran is approved for adolescents ≥12 years with HeFH or HoFH with residual LDLR function and is under investigation in younger children.
- Other PCSK9‑targeting therapies (lerodalcibep, enlicitide) are in clinical trials from 6 years of age.
- Among bile acid sequestrants, colesevelam is best tolerated but should be reserved for situations where newer LLTs are unavailable or not tolerated.
- Bempedoic acid has completed a phase 2 trial in children with HeFH aged 6–17 years.
If LDL‑C goals are not achieved with guideline‑recommended statin doses and PCSK9 inhibitors are unavailable, use maximally tolerated statin plus ezetimibe, a cholesterol-lowering diet, and consider bile acid sequestrants if available.
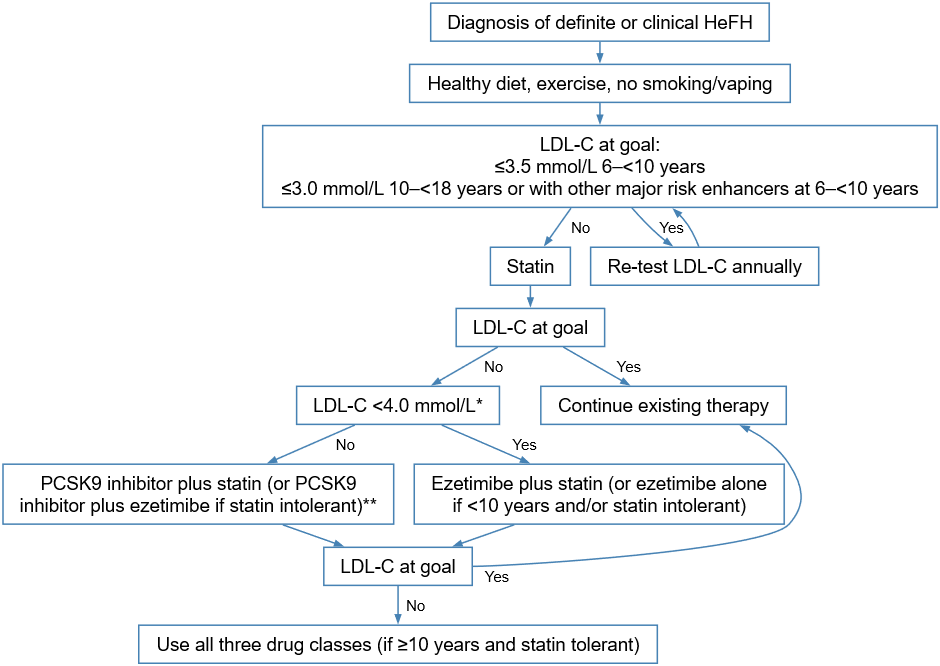
*Ezetimibe reduces low-density lipoprotein-cholesterol (LDL-C) concentrations in statin-treated children by ~15% (Table 3), which may be sufficient when LDL-C <4.0 mmol/L. If greater reductions are needed to achieve the treatment goal, add PCSK9 inhibitors to statin treatment (or to ezetimibe if a child is statin intolerant). Only in rare cases should three drugs be used.
**PCSK9 inhibitors are approved for children with FH from 8 years (alirocumab) or 10 years (evolocumab) or 12 years (inclisiran; FDA approved). To convert LDL from mmol/L to mg/dL, multiply the mmol/L value by 38.67.
Does sex matter?
Men with FH have a higher risk of developing premature ASCVD. However, women with FH have higher LDL-C exposure at a young age owing to higher LDL-C in childhood and interruptions in treatment for family planning, pregnancy, and breastfeeding. On average, women with FH have 2.3 years pregnancy related off-treatment time. Therefore, it is crucial to begin treatment as early in girls as in boys to address this increased LDL-C burden.
Safety
Side effects from statins in children are generally less frequent than in adults. Muscle symptoms are the most common reported side effect of statins overall, but studies indicate that these symptoms in adults are likely not caused by statin therapy. Increases in creatine kinase or liver enzymes are rare in children.
While statins in adults slightly raise the risk of new-onset diabetes, changes in insulin sensitivity have not been observed in children and adolescents after up to 7 months of treatment. Although a long-term risk of diabetes in children who start on statins from an early age cannot be ruled out, the cardiovascular benefits strongly outweigh this potential risk. The potential risk highlights the need to promote a healthy lifestyle to prevent obesity in children with FH.
- Ezetimibe is well tolerated in young people, with side effects similar to placebo or statin alone.
- Bile-acid sequestrants may lead to gastrointestinal issues.
- Evolocumab and alirocumab have been tested in children with HeFH and were generally well tolerated, with injection site reactions being the most common side effect. No issues were reported related to liver and muscle function, growth, puberty, neurocognition, glucose homeostasis, liposoluble vitamins, or steroid hormones, and no anti-drug antibodies developed.
- Inclisiran also appears well tolerated, with injection site reactions being the most common side effect.
- Long-term data on PCSK9 inhibitors in children is lacking.