Lp(a) Awareness Day 2026
Welcome to Lp(a) Awareness Day 2026! We’re excited to present this special website, dedicated to providing you with the latest updates and insights on lipoprotein(a)
Join us as we unite to increase awareness, promote education, and support efforts to improve health outcomes associated with Lp(a). Find more information using the hashtags: #KnowLpa and #LpaAwarenessDay.
Let’s make Lp(a) Awareness Day 2026 a truly impactful event!
What is Lp(a) Awareness Day?
Launched in 2022 to raise awareness of elevated lipoprotein(a), also known as elevated Lp(a) and pronounced: “l-p-little-A”. High Lp(a) concentration is one of the most important causal risk factors for cardiovascular disease (CVD).
Through our international network and collaboration with FH Europe Foundation, as well as social media engagement, we will draw attention to this important inherited disorder and encourage everyone to join the movement.
By sharing important information, we can empower all stakeholders to spread the word about high Lp(a) as an under-recognised cause of premature heart disease and stroke.
Why do we need Lp(a) Awareness Day?
- Globally 1 in 5 people are estimated to have elevated levels of Lp(a) which are an independent cardiovascular disease (CVD) risk factor.
- This makes an estimated population of 1.4 billion people globally. Despite this, the contribution of elevated Lp(a) concentration to CVD risk remains underappreciated.
- Most people have never heard of Lp(a)
- Only 1-2% of the population has had an Lp(a) measurement and therefore most of those with elevated concentrations do not know about their increased levels.
- To highlight fact that the 2025 Focused Update of the 2019 ESC/EAS Guidelines for the Management of Dyslipidaemias exists and must be used.
Help us raise awareness
Take action and help us raise awareness about this common genetic condition causing early heart disease and stroke.
Thanks to FH Europe Foundation, you can download the social media posts in over 20 languages:
Arabic, Chinese, Croatian, Czech, Dutch, French, English, German, Greek, Hebrew, Hungarian, Italian, Japanese, Latvian, Polish, Portuguese (Brazilian and European), Romanian, Serbian, Slovenian, Spanish and Urdu.
What is Lp(a) International Task Force?
The discourse on Lp(a) among many stakeholders across the globe (medical societies, healthcare professionals, academics/researchers, patient organisations and life sciences industry) points to the urgent need to encourage a more systematic and structured approach to testing the population, following guidelines, to decrease the overall cardiovascular disease (CVD) risk / prevent CVD from high levels of Lp(a). Recommendations and guidelines such as the EAS Lipoprotein(a) 2022 Consensus Statement[1] underline that everyone should be tested once in a lifetime. An enabling policy environment is crucial for governments to be able to deliver on CVD prevention, health innovation, and to ensure optimal and swift access to preventative therapies for individuals and relatives affected with elevated Lp(a).
Effective identification of Lp(a) levels as an independent and causal risk factor for CVD[2] and management options, including imminent new medicines, will address a clear Unmet Medical Need (UMN), and sustainability of health systems.
To tackle this, FH Europe Foundation embarked on the preparation of an ambitious global strategy and roadmap on Lp(a). In April of 2023, a core team was established with the objective of setting up an International Task Force (ITF) of experts from several different disciplines to contribute to this. This Task Force met for the first time in June and will finalise its work at a face-to-face meeting in the framework of the ESC Congress in Amsterdam at the end of August 2023. The aim was to launch in January 2024 a 5-year project to implement a global strategy and roadmap for Lp(a) testing.
However, a key milestone before that is a Scientific Summit in the framework of the United Nations General Assembly, during which FH Europe Foundation will present the need for much more policy attention to the global burden of Lp(a) and how this can be effectively tackled, to save lives, and also to reduce pressure on overstretched health systems.
[1] https://eas-society.org/page/lipoproteina-consensus-2022/
[2] Doherty S, Hernandez S, Rikhi R, et al. Lipoprotein(a) as a Causal Risk Factor for Cardiovascular Disease. Curr Cardiovasc Risk Rep. 2025;19(1):8. doi:10.1007/s12170-025-00760-1
Ground-Breaking International Study on Lp(a) Testing Cost Effectiveness
A Hidden Heart Risk Affects 1 in 5 – And a Simple Blood Test Could Help Stop It
A new study* shows routine testing for a little-known cardiovascular threat could prevent heart attacks, strokes, and save millions in health costs.
Most people have heard of cholesterol. But there’s another dangerous lipid in the blood – lipoprotein(a), or Lp(a), which if high in levels, could be silently putting millions at risk.
An international study led by Professor Zanfina Ademi and her Team at Monash University (Melbourne, Australia) reveals the cost effectiveness of testing high levels of Lp(a), a genetic and lifelong risk factor for heart disease affecting nearly 1 in 5 adults.
“This is one of the biggest blind spots in heart health,” said Professor Zanfina Ademi, a health economist and senior author of the study. “You can have a healthy lifestyle and normal cholesterol, but if your Lp(a) is high, you’re still at serious risk.”
Cardiovascular disease remains the world’s leading cause of death. In Australia, it costs over $14 billion a year; in Europe, that number soars to €282 billion. Yet Lp(a), which cannot be improved by diet or exercise, is not part of routine testing in most healthcare systems.
Published in Atherosclerosis, the study analysed data from over 10,000 adults in the UK. The results were striking: routine Lp(a) testing would have reclassified 20% of participants as high-risk, leading to earlier intervention with blood pressure or cholesterol-lowering medications.
In the same issue, Prof. Jan Boren, Editor-in-Chief of Atherosclerosis, issues a call to action in an editorial**, urging guideline developers and policymakers to act: “When a simple blood test can help prevent life-threatening cardiovascular events and improve quality of life, all in a cost-effective way, implementing such testing isn’t just advisable, it’s imperative”.
The modelling showed that, testing could prevent 60 heart attacks, 13 strokes and 26 early deaths (per 10,000 people tested). While adding 217 years and 255 years of healthy life – all while saving approximately $85 and £263 per person in Australia and in the UK respectively in medical and productivity costs. Researchers tested this approach in nine high income countries and found the same result everywhere: regularly testing for Lp(a) could save money in all their healthcare systems.
“This is a game-changer,” said Professor Florian Kronenberg of the Medical University of Innsbruck, Chair of the Lp(a) International Taskforce. “A one-time test could prevent countless tragedies and is one of the most cost-effective tools we have.”
The research helped inform the Brussels International Declaration on Lp(a) Testing and Management, a new global policy roadmap calling for Lp(a) to be included in national cardiovascular screening programs.
Magdalena Daccord, CEO of FH Europe and co-author of the study, said: “Most people think they’re safe if their cholesterol is normal. But Lp(a) is often the missing piece. This simple test can save lives. The science is here – now it’s time to act.”
Commissioned by the Lp(a) International Taskforce and hosted by the FH Europe Foundation (FHEF), this patient-driven research initiative was led by the Centre for Medicine Use and Safety at the Monash Institute of Pharmaceutical Sciences, in collaboration with global researchers and the Lp(a) International Taskforce. The study forms part of a broader multistakeholder effort to advance understanding and action on Lp(a).
* Lp(a) testing for the primary prevention of cardiovascular disease in high-income countries: a cost-effectiveness analysis. Jedidiah I Morton, Florian Kronenberg, Magdalena Daccord, Nicola Bedlington, Marius Geantӑ, Tobias Silberzahn, Zhenyue Chen, Jean-Luc Eiselé, Bogi Eliasen, Mariko Harada-Shiba, Marc Rijken, Albert Wiegman, George Thanassoulis, Pia R Kamstrup, Iñaki Gutiérrez-Ibarluzea, Pablo Coral, Raul D Santos, Erik Stroes, Michal Vrablík, Gerald F Watts, Christie M Ballantyne, Samia Mora, Børge G Nordestgaard, Kausik K Ray, Stephen J Nicholls, Zanfina Ademi, On behalf of the Lp(a) International Taskforce (ITF) initiative.
Why the Safe Hearts Plan matters on Lp(a) Awareness Day?

On Lp(a) Awareness Day, we highlight the importance of early detection and prevention of elevated lipoprotein(a), a common but often overlooked inherited risk factor for cardiovascular disease. Lp(a) levels are largely determined by genetics, remain stable throughout life, and are not detected in standard cholesterol tests – making targeted, one-time testing essential.
High Lp(a) can significantly increase the risk of heart attack, stroke, and aortic valve disease, even in otherwise healthy individuals. Because it is present from birth, early identification allows for timely risk assessment and preventive measures to reduce long-term cardiovascular damage.
The European Commission’s Safe Hearts Plan, published in December 2025, is the first EU-wide initiative to take a comprehensive approach to cardiovascular disease. Crucially, it explicitly recognises elevated Lp(a) as a key inherited risk factor. By promoting early-life screening, personalised prevention, and improved awareness, the Plan creates a real opportunity to identify individuals at risk sooner and intervene before serious disease develops.
In the context of Lp(a) Awareness Day, the Plan reinforces that early identification and intervention are not just best practice – they can be lifesaving. It sets a clear direction for Europe to move from reactive, late-stage treatment to proactive, lifelong cardiovascular care.
Consensus & Clinical Guidance
- Lipoprotein(a) in atherosclerotic cardiovascular disease and aortic stenosis: a European Atherosclerosis Society consensus statement
Florian Kronenberg, Samia Mora, Erik S.G. Stroes et al.
European Heart Journal, Volume 43, Issue 39, 14 October 2022, Pages 3925–3946, https://doi.org/10.1093/eurheartj/ehac361
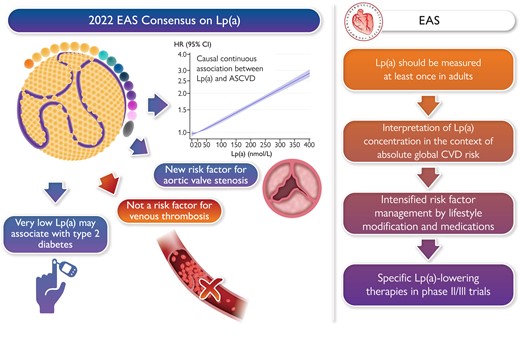
More than a decade after first highlighting Lp(a), the European Atherosclerosis Society (EAS) has published an updated consensus statement. This 2022 statement brings together extensive evidence for elevated Lp(a) concentration as a causal risk factor for atherosclerotic cardiovascular disease (ASCVD), irrespective of gender and ethnicity, as well as for aortic valve stenosis, and provides practical guidance on testing and treating high Lp(a) levels.

- Women, lipids, and atherosclerotic cardiovascular disease: a call to action from the European Atherosclerosis Society
Roeters van Lennep JE, Tokgözoğlu LS, Badimon L, Dumanski SM, Gulati M, Hess CN, Holven KB, Kavousi M, Kayıkçıoğlu M, Lutgens E, Michos ED, Prescott E, Stock JK, Tybjaerg-Hansen A, Wermer MJH, Benn M.
European Heart Journal, Volume 44, Issue 39, 14 October 2023, Pages 4157–4173, https://doi.org/10.1093/eurheartj/ehad472
Cardiovascular disease is the leading cause of death in women and men globally, with most due to atherosclerotic cardiovascular disease (ASCVD). Despite progress during the last 30 years, ASCVD mortality is now increasing, with the fastest relative increase in middle-aged women. Missed or delayed diagnosis and undertreatment do not fully explain this burden of disease. Sex-specific factors, such as hypertensive disorders of pregnancy, premature menopause (especially primary ovarian insufficiency), and polycystic ovary syndrome are also relevant, with good evidence that these are associated with greater cardiovascular risk. This position statement from the European Atherosclerosis Society focuses on these factors, as well as sex-specific effects on lipids, including lipoprotein(a), over the life course in women which impact ASCVD risk. Women are also disproportionately impacted (in relative terms) by diabetes, chronic kidney disease, and auto-immune inflammatory disease. All these effects are compounded by sociocultural components related to gender. This panel stresses the need to identify and treat modifiable cardiovascular risk factors earlier in women, especially for those at risk due to sex-specific conditions, to reduce the unacceptably high burden of ASCVD in women.
- Lp(a) – what is new in the 2025 Focused Update on the 2019 ESC/EAS Guidelines for the management of dyslipidaemias?
Whether lowering Lp(a) reduces the risk of ASCVD and AVS progression has yet to be shown; the extent of Lp(a) lowering required for clinical benefit is also not known. In the absence of specific Lp(a)-lowering therapies, early risk factor management and more intensive LDL-C lowering is reasonable, considering both absolute CV risk and Lp(a) levels.
Although small studies have suggested that statins may have a slight Lp(a) increasing effect, individual-level data on participants in seven randomized, placebo-controlled, statin outcome trials found that statins had no effect on Lp(a) concentrations. Therefore, clinical decision-making should be influenced by the degree of Lp(a) elevation and the patient’s other risk factors, and patients with high levels of Lp(a) should be strongly encouraged to take or continue to take high-intensity statins if their risk is sufficiently high.
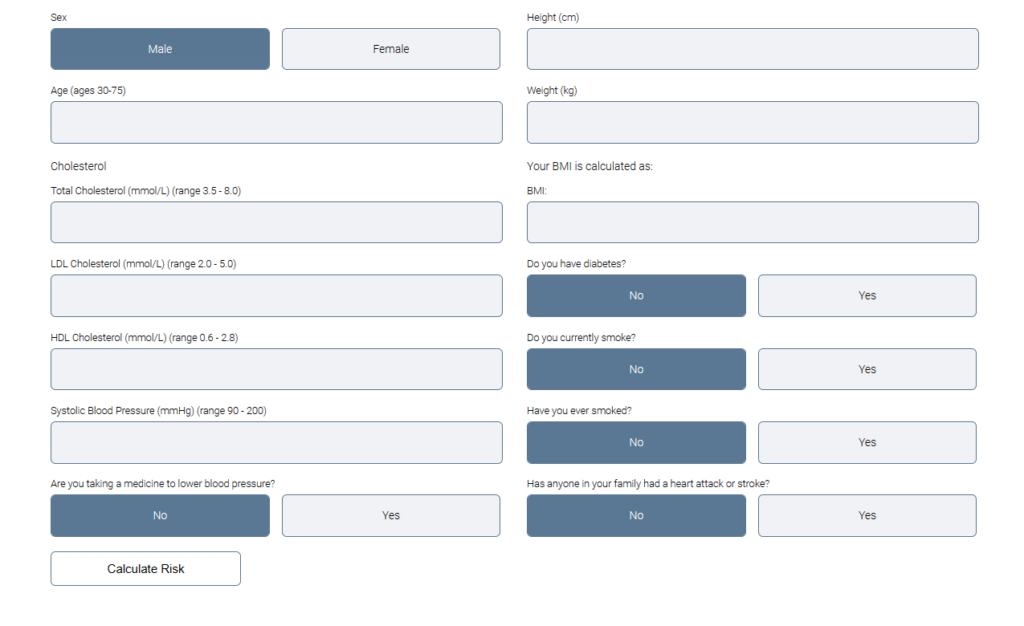
- Lp(a) Clinical Guidance – estimating the risk of heart attack & stroke caused by Lp(a)
Lp(a) Clinical Guidance is a website, launched in connection with the EAS Consensus position paper on Lp(a). It is intended for use by the general public, to help them understand their Lp(a) levels, and by clinicians, to help them better manage their patients with elevated Lp(a).
Lp(a) Clinical Guidance will help you determine how much your Lp(a) level increases your risk of having a heart attack or stroke and also provide you with specific guidance about what you can do to lower your risk if your Lp(a) level is elevated.
Talks on Lp(a)
- Lp(a) – Finding the right place
- Lp(a) – who to measure and what to do about it?
- What do we need to do? A call to action on Lp(a) testing
- EAS/ESC Guidelines: Lipoprotein(a) – guideline updates and clinical case
- The Cost-Effectiveness of Lp(a) testing and the Brussels International Declaration
- Ask me anything about Lp(a)
NEW! Certificate in Lipidology – CME-accredited
Professionals working in lipid clinics often face challenges in managing atherosclerotic vascular disease in daily practice.
This programme will help you address these challenges by improving your understanding of lipid disorders and cardiovascular risk assessment, and by strengthening your ability to support patients with lifestyle changes and treatment adherence.
The course also offers practical guidance on managing patients with atherosclerotic vascular disease and inherited lipid disorders, with contributions from clinicians, researchers, nurses, and patients.
The CME-accredited programme awards 4 CME credits upon completion.
Key scientific publications
Over the past year, Atherosclerosis has published several landmark articles that substantially advance our understanding of lipoprotein(a), from epidemiology and risk modification to policy, economics and therapeutic implications. The papers highlighted in this newsletter were selected for the Lp(a) Awareness Day because together they cover the full translational spectrum—clarifying who to test, how often, how Lp(a) interacts with inflammation and comorbidities, and what current and future therapies can realistically achieve, thereby directly informing clinical practice and European cardiovascular prevention strategies.
The Brussels International Declaration on Lp(a) Testing and Management

This declaration, co‑created by the Lp(a) International Task Force and key global stakeholders at the 2025 Lp(a) Global Summit, responds to the paradox of strong causal evidence for Lp(a) as a cardiovascular risk factor but very low testing rates (1–2%) despite a prevalence of elevated Lp(a) in roughly 1 in 5 individuals. It calls for integration of Lp(a) into global and national cardiovascular health plans, political commitment to at least once‑in‑a‑lifetime reimbursed testing, and investment in education for professionals and the public, thereby positioning Lp(a) as a core component of future cardiovascular prevention policy. It is in line with the ideas of the EU Safe Hearts Plan.
To the full articleLp(a) testing for the primary prevention of cardiovascular disease in high-income countries: a cost-effectiveness analysis
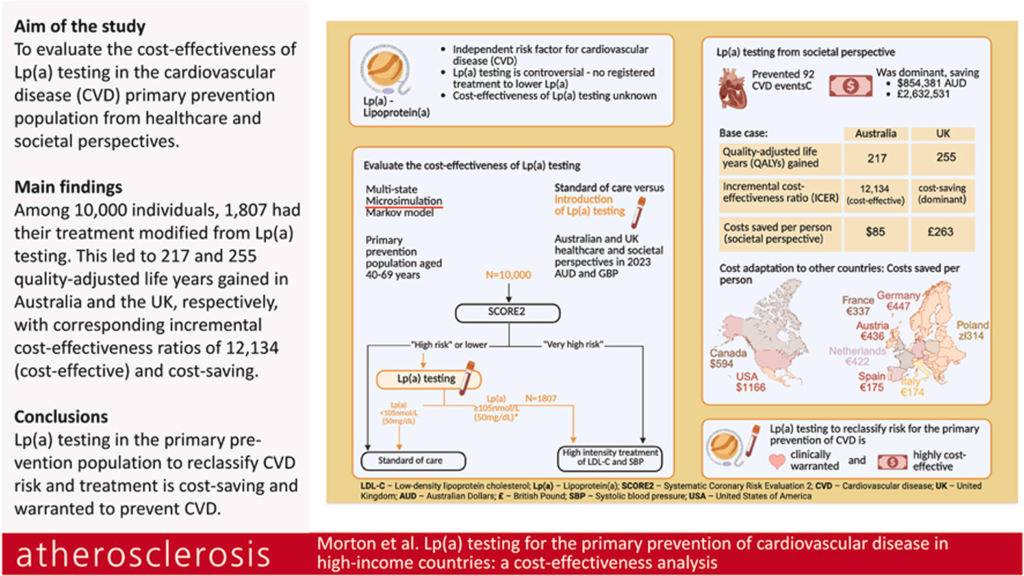
Morton et al. asked a simple question: if we measure Lp(a) once in people without known heart disease, does it pay off to treat those with high levels more intensively? They used real‑world data from a large population study and computer modelling to show that identifying people with high Lp(a) and starting them on cholesterol‑ and blood pressure‑lowering medication would prevent many heart attacks and strokes and gaining quality-adjusted life years, while actually saving money for health systems over time. This study was an important Basis for the key asks of the Brussels International Declaration on Lp(a) Testing and Management.
To the full articleEffect of lipid-lowering therapies on lipoprotein(a) levels: a comprehensive meta-analysis of randomized controlled trials
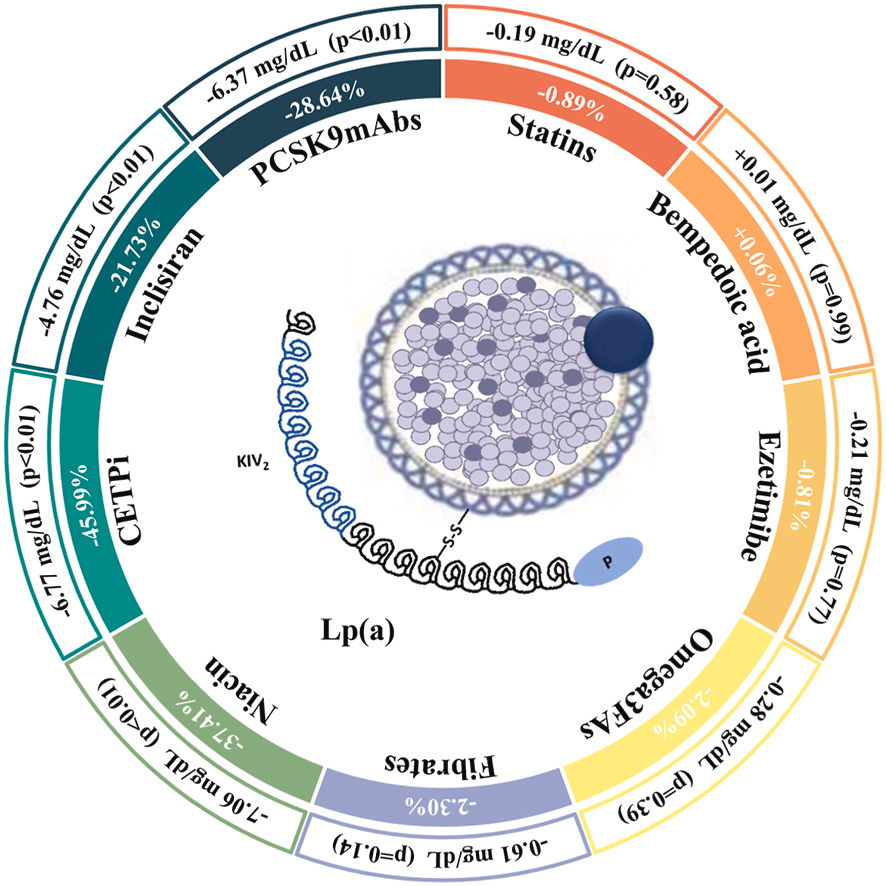
This comprehensive meta‑analysis of 147 randomised trials (145,314 participants) shows that most standard lipid‑lowering agents (statins, bempedoic acid, ezetimibe, omega‑3s, fibrates) do not materially change Lp(a), whereas PCSK9 monoclonal antibodies (≈29% reduction), inclisiran (≈22%), and CETP inhibitors (≈46%) significantly lower Lp(a), with greater absolute reductions at higher baseline levels. By systematically quantifying the Lp(a) effects of current and emerging therapies, the study both clarifies realistic expectations from available agents and underscores the need for dedicated Lp(a)‑targeted drugs and outcome data.
To the full articleAssociation of Lipoprotein(a) with cardiovascular events among individuals with autoimmune conditions
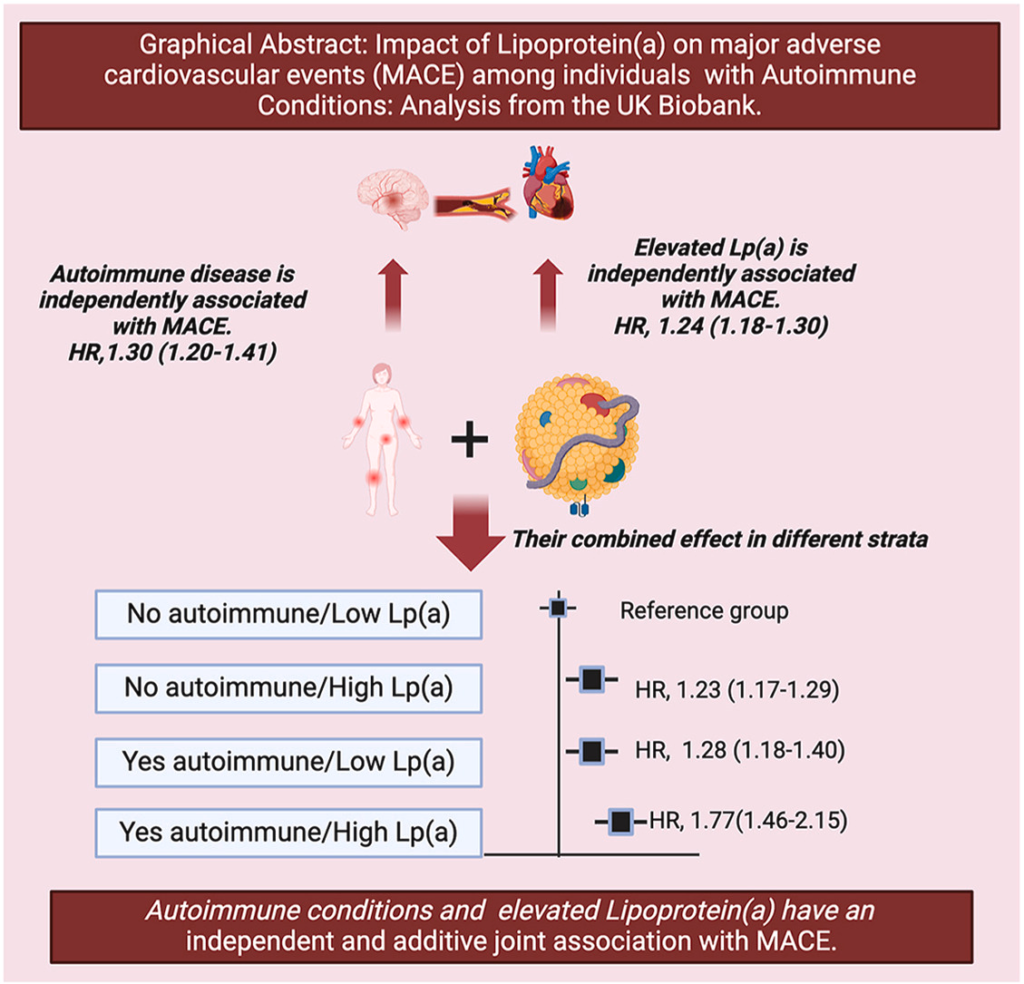
Using UK Biobank data from 353,035 participants (11,229 with autoimmune conditions), this analysis demonstrates that autoimmune status (HR 1.30) and elevated Lp(a) ≥125 nmol/L (HR 1.24) independently increase MACE risk, with an additive joint hazard ratio of 1.77 for those with both. The absence of a statistical interaction but clear additive risk supports considering Lp(a) in the vascular risk assessment of patients with autoimmune disease, and highlights them as a priority group for future Lp(a)‑lowering interventions in high‑risk primary prevention.
To the full articleInterleukin-6 modifies Lipoprotein(a) and oxidized phospholipids associated cardiovascular disease risk in a secondary prevention cohort
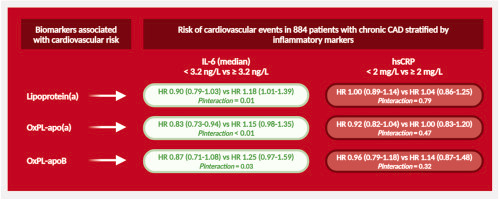
In patients with chronic coronary syndrome from the placebo arm of the low‑dose colchicine 2 trial, Lp(a), OxPL‑apo(a) and OxPL‑apoB were associated with cardiovascular events only in those with elevated IL‑6, but not in those with lower IL‑6 or when stratified by hsCRP. These findings suggest that low‑grade inflammation marked by IL‑6, rather than hsCRP, modifies the risk conferred by Lp(a) and OxPL, supporting a more nuanced risk stratification that integrates inflammatory pathways with Lp(a) biology in secondary prevention.
To the full articleLCN Lp(a) webinar series on-demand
Explore our series of five Lp(a) webinars, which cover topics such as what Lp(a) is, how to measure it, recommendations for screening, therapeutic approaches, and the practical implications of these findings.
LCN Lp(a) webinar series available on-demandEAS Academy
At EAS Academy, we have gathered all educational resources on this topic, including:
- EAS Congress sessions
- Expert lectures and webinars
EAS Lipid Clinic Network
The EAS Lipid Clinic Network (EAS-LCN) is a global collaborative network connecting lipid clinics and healthcare professionals dedicated to the prevention, diagnosis, and management of lipid disorders. The network promotes high-quality, equitable patient care worldwide through harmonisation, education, and knowledge exchange.
To the Lipid Clinic NetworkAtheroTalk episodes
AtheroTalk episodes feature concise expert interviews and discussions with leading researchers and clinicians in the field of lipidology.
Listen to our experts