
Lp(a)
What is new?
Whether lowering Lp(a) reduces the risk of ASCVD and AVS progression has yet to be shown; the extent of Lp(a) lowering required for clinical benefit is also not known. In the absence of specific Lp(a)-lowering therapies, early risk factor management and more intensive LDL-C lowering is reasonable, considering both absolute CV risk and Lp(a) levels.
An online Lp(a) risk and benefit algorithm is available at http://www.eas-society.org/LPA_risk_and_benefit_algorithm
Although small studies have suggested that statins may have a slight Lp(a) increasing effect, individual-level data on participants in seven randomized, placebo-controlled, statin outcome trials found that statins had no effect on Lp(a) concentrations. Therefore, clinical decision-making should be influenced by the degree of Lp(a) elevation and the patient’s other risk factors, and patients with high levels of Lp(a) should be strongly encouraged to take or continue to take high-intensity statins if their risk is sufficiently high.
Recommendations
| Recommendations | Classa | Levelb |
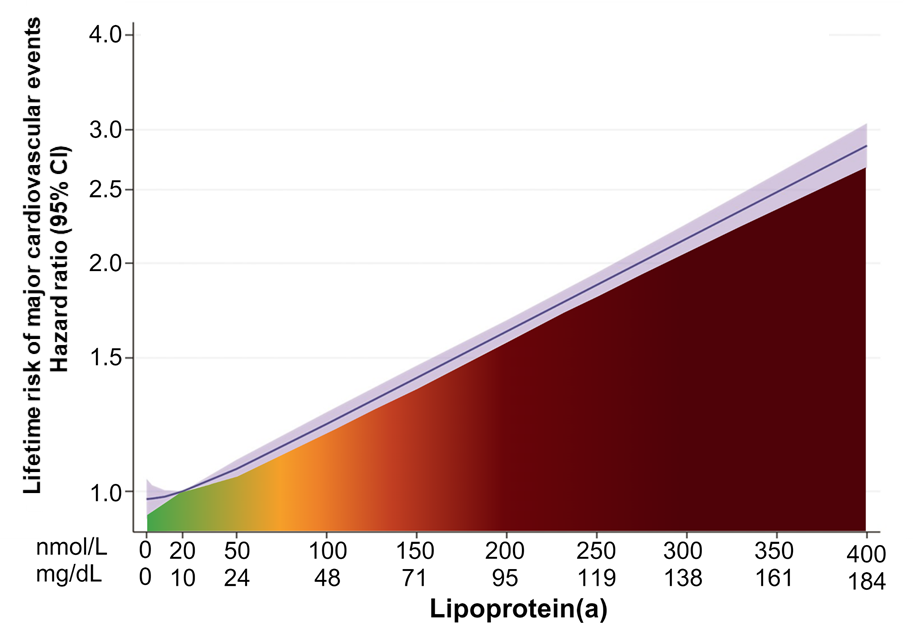
| Lp(a) levels above 50 mg/dL (≈105 nmol/L) should be considered in all adults as a CV risk-enhancing factor, with higher Lp(a) levels associated with a greater increase in risk.37,100 | IIa | B |
CV, cardiovascular; Lp(a), lipoprotein(a).
a Class of recommendation.
b Level of evidence.